
Perfusion Pressure
Increasing preload with fluid administration is recommended, as it is better to have the patient in optimal condition before the heart is lifted. Once this has been accomplished, the addition of steep Trendelenburg seems to help.34 Communicate with the surgeon as to how much manipulation the heart can tolerate when he/she immobilizes the surface of the heart. Alpha agents such as phenylephrine are recommended as the first choice because they increase the afterload and restore the blood pressure without markedly increasing the myocardial oxygen consumption. Although the hypotension is not caused by decreased afterload but rather low cardiac output and preload, alpha agents are used as a temporizing measure. However, because the patient's condition may rapidly deteriorate, be prepared to administer much more potent agents such as epinephrine and norepinephrine.
Stabilization Devices
The type of device used by the surgeons to immobilize the surgical field can make a difference.35 You can see in the picture below the marked compression produced by a fork-like stabilizer being used on an anastomosis on an LAD. It has been documented that compression devices cause a reduction in cardiac output.35
 |
| Figure 8. Compression Device on Heart (photo courtesy of Dr. Luis Michelsen, Emory University Medical Center, Atlanta, GA) |
 |
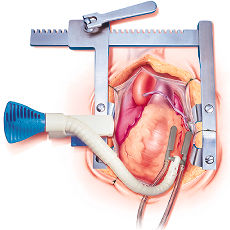
| Figure 9. Octopus® 2 on Heart |
Suction devices stabilize the target area with less hemodynamic changes than compression devices.35,36 Suction devices leave round areas of ecchymosis. The lesions are superficial and transient. Studies in animals show complete resolution without scarring and that the coronary arteries are not affected.34
Low Cardiac Output
Cardiac output may be markedly
lowered during this procedure due to compression and decreased contractility
from beta-blockers, ischemia, and heart displacement. The consequences
can be very severe for the brain, intestines, kidneys and other organs
that require high blood flow. There is debate among anesthesiologists
about the best way to monitor
cardiac output (CO) during this procedure. Some recommend PA catheters
that can monitor mixed venous oxygen saturation (SVO2)
on every patient. We rely mainly on the echocardiogram as a global monitor
of ventricular function. Just like in cardiopulmonary resuscitation
(CPR), end-tidal CO2 (ETCO2) can be a useful
indicator of global circulation during periods of hemodynamic instability.
If the surgeon is manipulating the heart and the systemic pressure is
not markedly affected but the ETCO2 is rapidly
declining, beware. Anecdotally, in two cases of cardiac arrest where
the ETCO2 curve remained close to normal throughout
the resuscitation efforts, the patients recovered.
|
|
||||||||||